New Clearer Look, Smoother Feel Means Better Patient Compliance
Our new clear formula Vella 5% sodium fluoride varnish with xylitol offers improved esthetics and smooth and easy application in four great-tasting flavors: strawberry, spearmint, melon and bubblgum. When your varnish application looks better, feels better in the mouth and tastes great, it's sure to improve patient compliance.
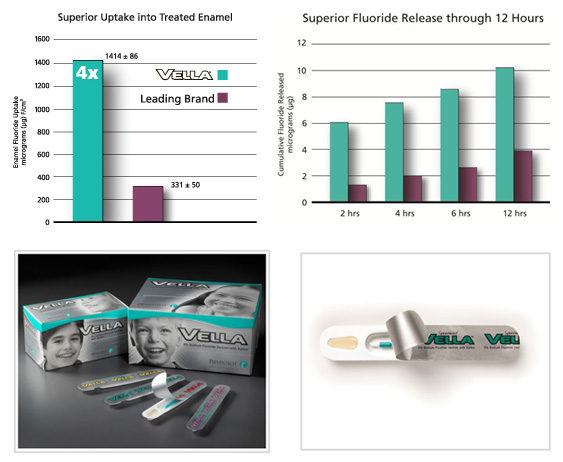
Vella's thin layer formula applies easier, with no clumps, lumps or stringy messes. And Vella sets quickly in saliva and has great fluoride uptake at two hours. Plus its n-Hexane free … Google it!
Ask your dealer for Vella Varnish today. Or call us at 1-800-474-8681 and we'll ship your order in your dealer's name.
Our Preventive Dental Care Products are Made in the USA








 Samples
Samples